

Peyronie’s disease is primarily caused by repetitive micro-trauma to the penis, which triggers an abnormal wound healing response, leading to the formation of fibrous scar tissue called plaque.
This condition, which affects far more men than official statistics suggest—with studies indicating over 1 in 10 men may have it, not just the 1 in 100 diagnosed—results in penile curvature, pain, and potential sexual dysfunction.
While injury is the leading theory, a combination of genetic predisposition, underlying connective tissue disorders, and other health factors like diabetes significantly contribute to its development. Understanding these root causes is the first step toward effective management and treatment.
For many men, a change in the shape of their penis is a source of significant anxiety and concern. It’s a topic shrouded in misunderstanding and often goes undiscussed.
This comprehensive guide, written with medical expertise, aims to demystify Peyronie’s disease.
We will delve deep into the scientific understanding of its causes, explore the full spectrum of risk factors, explain the symptoms and diagnostic process, and provide a clear overview of modern treatment options.
Our goal is to empower you with authoritative, trustworthy information to navigate this challenging condition.
In This Article
What is Peyronie’s Disease, Exactly?
Peyronie’s (pay-roe-NEEZ) disease is a non-cancerous condition resulting from the formation of fibrous scar tissue, known as plaque, that develops in the deep tissue under the skin of the penis.
This plaque is not the same as the plaque that builds up in arteries. It is a benign, localized area of fibrosis that can cause pain, penile curvature or bending, and in some cases, erectile dysfunction (ED).
A Simple Definition for Patients
Imagine the penis has an internal elastic sleeve that allows it to stretch and become rigid during an erection.
In Peyronie’s disease, a small, tough, and inelastic patch—like a tiny internal scar—forms on this sleeve.
When an erection occurs, the rest of the sleeve stretches normally, but the scarred patch does not.
This tethering effect forces the penis to bend or curve, often causing pain and making intercourse difficult or impossible.
The Science Behind the Curve: Tunica Albuginea and Plaque
To understand the cause of Peyronie’s disease, it’s crucial to know a little about penile anatomy.
The penis contains two sponge-like chambers called the corpora cavernosa, which fill with blood to create an erection.
These chambers are wrapped in a strong, elastic sheath of tissue called the tunica albuginea.
In Peyronie’s disease, the plaque forms directly on this tunica albuginea. As the plaque matures, it loses its elasticity.
The location of the plaque determines the direction of the curve. If the plaque is on the top of the penis (the most common location), it will curve upwards. If it’s on the bottom, it will curve downwards, and so on.
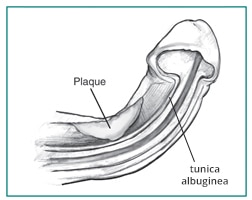
A diagram from the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) illustrating how plaque on the tunica albuginea causes penile curvature.
Is it Cancer? Debunking Common Myths
One of the first fears many men have when they feel a lump on their penis is cancer. It is essential to state this clearly: Peyronie’s disease is not cancer, nor is it a tumor.
The plaque is a benign (non-cancerous) buildup of scar tissue. It does not spread to other parts of the body and is not life-threatening.
However, its impact on quality of life, mental health, and sexual function can be profound, which is why seeking a medical diagnosis is so important.
How Does Peyronie’s Disease Develop? The Two Phases
Peyronie’s disease is not a static condition, it evolves over time, typically in two distinct phases.
Understanding which phase you are in is critical because it directly influences treatment decisions.
The Acute Phase: Inflammation and Onset of Symptoms
The acute phase is the initial, active stage of the disease. This is when the plaque is forming and inflammation is present.
According to guidelines from the American Urological Association (AUA), this phase can last anywhere from 5 to 18 months.
During the acute phase, you may experience:
- Penile Pain: This is a hallmark of the acute phase, often occurring with or without an erection. The pain is due to active inflammation.
- Developing Curvature: The bend or curve in the penis begins to appear and may progressively worsen during this time.
- Plaque Formation: You may begin to feel a nodule or hard lump on the penis.
Medical treatments during this phase, such as injections or traction therapy, are often aimed at reducing inflammation, managing pain, and potentially preventing the curvature from getting worse.
The Chronic Phase: Stabilization and Long-Term Changes
The chronic phase begins when the inflammation subsides and the plaque stabilizes.
This typically occurs 12 to 18 months after symptoms first appear.
In this phase, the disease is no longer actively progressing.
Key characteristics of the chronic phase include:
- Stabilized Curvature: The penile curve stops getting worse.
- Reduced Pain: The pain associated with erections usually lessens or disappears completely.
- Hardened Plaque: The plaque is now a dense, calcified scar.
- Erectile Dysfunction (ED): ED that may have started in the acute phase can persist or worsen.
Surgical intervention is generally reserved for the chronic phase, once the deformity has been stable for at least 3-6 months.
This ensures that the correction will be lasting and not undone by further disease progression.
Can Peyronie’s Disease Go Away on Its Own?
While it is the hope of many, spontaneous resolution of Peyronie’s disease is rare.
The NIDDK notes that in a very small number of cases, the condition can resolve without treatment.
However, for the vast majority of men, the condition will either remain stable or worsen during the acute phase before stabilizing.
Relying on spontaneous improvement is not a recommended strategy, early consultation with a urologist is always the best course of action.
What Are the Primary Causes of Peyronie’s Disease?
While the exact trigger for Peyronie’s disease is not known with 100% certainty, medical experts have identified a leading theory and several major contributing factors.
The condition is believed to be multifactorial, meaning it’s likely a combination of injury, genetics, and other health issues.
Penile Trauma: The Leading Theory
The most widely accepted theory is that Peyronie’s disease results from an “aberrant wound healing” process following trauma to the penis.
This trauma doesn’t have to be a single, major event. It can be:
- Acute Injury: A direct blow to the penis or an incident during sexual activity where the erect penis is bent forcefully. This can cause bleeding within the layers of the tunica albuginea.
- Chronic Micro-Trauma: This is more common and often goes unnoticed. It involves repeated, minor injuries to the penis over time, perhaps from vigorous sexual intercourse or certain athletic activities.
In a normal healing process, the body would repair this damage without issue.
However, in men who develop Peyronie’s disease, the healing response is disorganized. Instead of forming normal, flexible tissue, the body deposits excessive amounts of collagen and fibrin, creating the hard, inelastic plaque.
As a review in the journal Reviews in Urology states, the etiology is “widely thought to involve minor penile trauma with subsequent aberrant wound healing”. This highlights the consensus in the medical community around the central role of injury and a faulty repair mechanism.
The Role of Genetics and Family History
Why do some men get Peyronie’s after an injury while others don’t? Genetics appear to play a crucial role. Both the NIDDK and Mayo Clinic confirm that having a close male relative (father or brother) with Peyronie’s disease increases your risk.
This suggests a hereditary predisposition to the abnormal fibrotic response.
Recent research published in 2025 in the Journal of Sexual Medicine has even begun to identify specific epigenetic differences in the penile tissue of men with Peyronie’s, suggesting that genetic expression, not just the genes themselves, is involved.
Autoimmune and Connective Tissue Disorders: A Systemic Link?
Peyronie’s disease is strongly associated with other conditions characterized by abnormal fibrosis or autoimmune responses.
This suggests that for some men, Peyronie’s is not just a localized penile issue but part of a broader, systemic tendency to form scar tissue.
Key associated disorders include:
- Dupuytren’s Contracture: A condition where tissue in the palm of the hand thickens and tightens, causing fingers to curl inward. This is the most common association. A 2025 study found a high prevalence of Peyronie’s disease in men with Dupuytren’s, particularly those with bilateral hand involvement.
- Plantar Fasciitis: Inflammation and thickening of the tissue on the bottom of the foot.
- Scleroderma: A group of autoimmune diseases that involve the hardening and tightening of the skin and connective tissues.
- Other Autoimmune Conditions: Systemic lupus erythematosus, Sjögren’s syndrome, and Behçet’s disease have also been linked to an increased risk of Peyronie’s disease.
Who is Most at Risk for Developing Peyronie’s Disease?
Beyond the primary causes, several well-established risk factors increase a man’s likelihood of developing Peyronie’s disease.
These factors often compound, creating a perfect storm for the condition to emerge.
The Impact of Aging
While Peyronie’s can occur at any age, its prevalence increases significantly with age. It is most common in men between 45 and 70.
As men get older, changes in the elasticity of their tissues can make the penis more susceptible to injury and less efficient at healing, increasing the chance of an abnormal fibrotic response.
Diabetes and Erectile Dysfunction: A Vicious Cycle?
Men with diabetes are at a significantly higher risk.
A landmark study cited by the NIDDK found that men with diabetes-associated ED have a 4 to 5 times higher chance of developing Peyronie’s disease.
Diabetes can cause vascular and nerve damage, contributing to both ED and poor wound healing, which are central to the development of Peyronie’s plaque.
Post-Prostate Cancer Surgery: An Underrecognized Risk
Men who have undergone a radical prostatectomy (surgical removal of the prostate) for prostate cancer have an increased incidence of Peyronie’s disease.
The exact reason is still being studied, but it’s believed to be related to post-surgical changes, including nerve damage and subsequent erectile dysfunction, which may lead to tissue changes and fibrosis.
Lifestyle Factors: Does Smoking or Vigorous Activity Play a Role?
While the direct link is less established than for other factors, some evidence suggests lifestyle can contribute.
Smoking is known to cause vascular damage and impair healing, which could theoretically increase the risk.
As mentioned earlier, vigorous sexual or nonsexual activities that can cause repeated micro-trauma are also a significant risk factor.
What Are the Telltale Symptoms of Peyronie’s Disease?
The signs and symptoms of Peyronie’s disease can appear suddenly or develop gradually.
They range from mild to severe and can have a major impact on sexual function and mental well-being.
The most common symptoms include:
- A Bend or Curve in the Penis: This is the defining characteristic. The penis may curve up, down, or to the side during an erection.
- Hard Lumps (Plaque): You may be able to feel flat lumps or a band of hard tissue under the skin of the penis. This is the scar tissue.
- Penile Pain: Pain, particularly during an erection, is common, especially in the acute phase of the disease. Some men may also feel pain when the penis is flaccid.
- Erection Problems (Erectile Dysfunction): Peyronie’s can make it difficult to get or maintain an erection. This can be due to pain, the mechanics of the curvature, or psychological distress.
- Shortening of the Penis: The inelastic plaque can prevent the penis from fully stretching during an erection, leading to a loss of length.
- Other Deformities: Some men develop an “hourglass” shape, where a narrow, tight band forms around the shaft, or indentations in the penis.
How Do Doctors Diagnose Peyronie’s Disease?
If you suspect you have Peyronie’s disease, the first step is to see a urologist, a doctor specializing in urinary and male sexual health.
The diagnosis is typically straightforward and based on your history and a physical exam.
Medical and Family History
Your doctor will ask detailed questions about your symptoms, when they started, whether you have pain, and if you recall any injury.
They will also ask about your family history and any other medical conditions you have, like diabetes or Dupuytren’s contracture.

Open communication with your healthcare professional is key to an accurate diagnosis and effective treatment plan.
Physical Examination
A urologist can usually feel the plaque in the penis, even when it is not erect.
To fully assess the deformity, your doctor may need to see the penis during an erection. This can be done in two ways:
- In-Office Injection: An injectable medicine is used to induce an erection in the doctor’s office. This allows the urologist to directly measure the curvature and assess the stability of the penis.
- At-Home Photos: You may be asked to take pictures of your erect penis at home from different angles to show the doctor at your follow-up visit.
Imaging Tests
In some cases, particularly if surgery is being considered, your doctor may order a penile Doppler ultrasound.
This test uses sound waves to create an image of the inside of the penis.
It can show the exact location and size of the plaque, check for calcification, and assess blood flow, which helps in planning the best course of treatment.
What Are the Treatment Options for Peyronie’s Disease?
The goal of treating Peyronie’s disease is to reduce pain, straighten the penis enough for satisfactory intercourse, and restore sexual function.
Treatment depends heavily on the phase of the disease (acute vs. chronic) and the severity of the symptoms.
Nonsurgical Treatments (Mainly for the Acute Phase)
During the active, inflammatory phase, treatments focus on managing symptoms and potentially slowing the disease’s progression.
- Oral Medications: Historically, various oral drugs have been tried, but the AUA guidelines state there is currently no oral medication that has been proven effective at reducing penile curvature. NSAIDs like ibuprofen may be recommended for pain.
- Injections: Injecting medication directly into the plaque is a primary treatment.
- Collagenase clostridium histolyticum (Xiaflex): This is the only FDA-approved medication for Peyronie’s disease. It’s an enzyme that breaks down the collagen that forms the plaque. It is approved for men with a curve greater than 30 degrees and is often combined with “modeling” (gentle bending) by the doctor.
- Verapamil: A blood pressure medication that may help by disrupting collagen production.
- Interferon: A protein that may help break down fibrous tissue and reduce pain.
- Traction Therapy: This involves using a mechanical device to stretch the penis for a set period each day. According to the Mayo Clinic, it is the only treatment shown to potentially improve penis length and is best started in the acute phase.
Surgical Treatments (For the Chronic Phase)
Surgery is the most effective treatment for correcting the curve but is only recommended for men in the chronic phase with a stable deformity that prevents sexual intercourse.
| Surgical Procedure | Best For | Pros | Cons |
|---|---|---|---|
| Plication Surgery | Less severe curves (<60 degrees), good erectile function. | – Simpler procedure – Lower risk of ED or numbness | – Causes some penile shortening – Does not restore lost length |
| Incision/Excision and Grafting | More severe curves (>60 degrees), complex deformities (e.g., hourglass). | – Straightens severe curves effectively – Can restore some lost length | – Higher risk of post-op ED – Potential for penile numbness – More complex surgery |
| Penile Implant (Prosthesis) | Men with both Peyronie’s disease and significant erectile dysfunction (ED). | – Corrects both the curve and the ED in one procedure – Provides a reliable erection | – Most invasive option – Risk of device infection or malfunction – Irreversible procedure |
Can Peyronie’s Disease Be Prevented?
Unfortunately, because the exact cause of Peyronie’s disease is not fully understood and involves a strong genetic component, there are no proven methods to prevent it.
Researchers have not found any link between diet, nutrition, or supplements and the prevention of this condition.
However, you can potentially reduce your risk of penile injury.
Being cautious during sexual activity, especially in positions that could cause the penis to bend, may help.
Additionally, managing underlying health conditions like diabetes is crucial for overall vascular and tissue health, which could indirectly play a role.
Frequently Asked Questions (FAQ)
1. Is Peyronie’s disease a sexually transmitted disease (STD)?
No. Peyronie’s disease is not contagious and cannot be transmitted to a sexual partner. It is a benign wound-healing disorder, not an infection.
2. Can masturbation cause Peyronie’s disease?
It is highly unlikely. The condition is linked to trauma that causes bleeding within the penile tissues. Normal masturbation does not typically generate this level of force. An aggressive or traumatic incident could theoretically contribute, but it is not a common cause.
3. Does Peyronie’s disease increase the risk of penile cancer?
No. The plaque associated with Peyronie’s disease is benign (non-cancerous) scar tissue. There is no evidence to suggest that having this condition increases your risk of developing penile cancer.
4. How common is Peyronie’s disease?
While diagnosed in about 1 in 100 men, studies suggest the true prevalence is much higher, likely affecting more than 1 in 10 men. Many men do not seek treatment due to embarrassment or mild symptoms.
5. Will I lose sensation in my penis after Peyronie’s surgery?
It’s a possible risk, especially with grafting surgery. Plication surgery has a lower risk of numbness. Penile implants generally preserve sensation in the skin and glans (head) of the penis. Discuss this risk thoroughly with your surgeon.
6. What is Xiaflex?
Xiaflex is the brand name for collagenase clostridium histolyticum, the only FDA-approved injectable medication for Peyronie’s disease. It is an enzyme that works by breaking down the collagen plaque that causes the curvature.
7. Can I still have children if I have Peyronie’s disease?
Yes. The disease does not affect sperm production or fertility. However, if the curvature is severe enough to make intercourse impossible, it can create a mechanical barrier to conception. Treatment can resolve this issue.
8. How long do I have to wait to have sex after surgery?
Your surgeon will give you specific instructions, but typically you will need to wait 4 to 8 weeks after surgery before resuming any sexual activity to allow the tissues to heal properly.
Conclusion
The journey with Peyronie’s disease often begins with confusion and anxiety, but it doesn’t have to end there.
We’ve established that this condition is primarily caused by an abnormal healing response to penile trauma, heavily influenced by genetics and other health factors.
It is a benign, non-cancerous disorder that progresses through an active acute phase before stabilizing into a chronic phase.
From nonsurgical options like Xiaflex injections and traction therapy to definitive surgical corrections, modern urology offers effective solutions to manage symptoms and restore sexual function.
The most critical step you can take is to overcome any hesitation and consult a urologist. Early diagnosis and intervention, especially in the acute phase, can lead to better outcomes.
If you have noticed a curve, pain, or lump, don’t wait. Schedule an appointment with a healthcare professional. You are not alone in this, and effective help is available.
We encourage you to share this article to help raise awareness and leave a comment below with any questions or to share your experience.
This article is for informational purposes only and does not constitute medical advice. The information contained herein is not a substitute for and should never be relied upon for professional medical advice. Always talk to your doctor about the risks and benefits of any treatment.